What works?
Motivational interventions
selected research articles
It is self-evident that motivation is a prerequisite of voluntarily making change. If I am enjoying my drinking or party drugs or smoking and I don’t seem to have any adverse consequences, then why am I going to change? Skilled use of motivational techniques can help people to change.
Meta-analysis :: 25 years of motivational interviewing
Lundahl BW, Kunz C, Brownell C, Tollefson D and Burke BL (2010) A Meta-Analysis of Motivational Interviewing: Twenty-Five Years of Empirical Studies. Research on Social Work Practice 20: 137-160
This meta-analysis included 119 studies covering a broad spectrum of addictive behaviours. MI was compared to weak interventions, such as being on a waiting list or treatment as usual, and strong interventions, such as a 12-step programme or CBT.
MI did not show significant benefits over strong interventions, which all have structure defined in some form of guidance, and so we consider only comparisons against weak interventions here. Motivational Enhancement Therapy was seen as a structured treatment defined as MI + feedback.
There were significant, small to moderate effects from MI for substance use problems (1st chart). There is evidence to support MI as an ‘additive’ or style of working with other interventions and also as a stand alone approach in preparation, a ‘prelude’ to other treatment or as MET (2nd chart). There is some evidence that more experienced and higher qualified staff get better results with MI.
Classic study :: commitment talk
Amrhein PC, Miller WR, Yahne CE, Palmer M & Fulcher L (2003). Client commitment language during motivational interviewing predicts drug use outcomes. Journal of Consulting and Clinical Psychology, 71: 862–878.
This is a detailed investigation of client talk from a single motivational interviewing (MI) session with 84 drug users. Analysis of the proportion of days abstinent (PDA) at intake and follow-up (3, 6, 9, 12 months) revealed three groups of users: ① high PDA at both intake and follow-up - maintainers; ② low PDA at intake and high at follow-up - changers; ③ low PDA at intake and low to moderate at follow-up - strugglers. Videotape recordings of the MI session were coded for frequency and strength of the client utterances (these were ‘thought units’ which could be a few words, phrases or sentences). Coded utterances were given a strength value: negative values indicating a wish to carry on using drugs and a positive value a wish to change.
The headline conclusion is that commitment talk is a useful final common pathway which brings together the processes of motivational dialogue and predicts outcomes. These were the main findings…
The kind of things said (coded) were the same for all three drug user groups. Commitment talk was most frequent, notably so at the start of sessions, followed by reasons for change, ability (self-efficacy), desire or need for change, and, least often, readiness to change. All change talk tended to reduce in frequency towards the end of sessions when action plans were discussed.
The strength of commitment talk differed between the three user groups at the start of the session. The maintainers had the strongest commitment, followed by changers and strugglers. By the end of the session the changers had reached the same strength of commitment as the maintainers, whereas the strugglers, despite a late-session increase in change talk, at the end became more entrenched in wanting to carry on using.
The talk coded as desire, ability, need and reason to change was not differentiated across the outcome groups. All four categories of talk tended to increase during a session, albeit self-efficacy was consistently low and the desire for change reduced when the discussion turned to how the treatment plan would work.
None of the talk coded as desire, ability, need and reason to change reliably predicted outcome categories and were strikingly bad at predicting poor outcomes; however, each contributed independently to commitment talk.
Strength of commitment talk reliably predicted the outcomes in 71 of 84 cases - 85% specificity (true negatives) and 92% sensitivity (true positives).
Note
This article does not describe how the strength of commitment talk was determined, albeit there are some examples of the kind of statements that would be rated with maximum positive and negative scores. Negative commitment scores would be seen as sustain talk, low positives as change talk, and high scores commitment talk.
Testing the MI model
It is clear that motivational interviewing can be applied to alcohol and drug addiction, behavioural addictions such as gambling, and pretty much any other kind of problem. Using MI as a stand alone typically produces modest outcomes and we suggest that practitioners adopt a motivational style of working; we have referred to this as using motivational dialogue.
Meta-analysis :: Testing the causal model of motivational interviewing
Magill, M., Gaume, J., Apodaca, T. R., Walthers, J., Mastroleo, N. R., Borsari, B., & Longabaugh, R. (2014) The Technical Hypothesis of Motivational Interviewing: A Meta-Analysis of MI’s Key Causal Model. Journal of Consulting and Clinical Psychology 82: 973–983
This meta-analysis included 16 studies where MI was the treatment for alcohol or drug misuse, smoking and gambling problems. The aim was to test the theoretical mode of action of motivational interviewing. MI consistent behaviour (eg open questions, reflections and affirmation) were compared to MI inconsistent behaviours (eg confrontations, warnings, unsolicited advice).
As predicted, MI consistent behaviour increased change talk but had uncertain effects on reducing resistance related talk and the outcome of treatment. MI inconsistent behaviour was clearly associated with less change talk, more resistance to change and poorer treatment outcome.
Important study :: Client perceptions of MI
Jones SA, Latchford G and Tober G (2016) Client experiences of motivational interviewing: An interpersonal process recall study. Psychology and Psychotherapy: Theory, Research and Practice 89: 97–114
Interviews with nine clients were conducted using interpersonal process recall (IPR), a methodology which utilises a video recording as a cue to aid memory recall. Clients watched a videotape of their MI session and were asked to identify and describe the important moments in the therapy session.
The aspects of therapy which clients in this study felt were important mirror those hypothesised to underlie the effectiveness of MI, including a non-confrontational approach, affirmation, and developing discrepancies between beliefs and behaviour.
The authors conclude these aspects are common to all therapies, as are the qualities of the therapist and the therapeutic relationship.
Important studies :: Analysis of the UK Alcohol Treatment Trial data
The following series of studies investigated the use of motivational techniques by therapists delivering Social Behaviour and Network Therapy (SBNT) or Motivational Enhancement Therapy (MET) in video recorded sessions in the UK Alcohol Treatment Trial to see what made a difference to service user responses and drinking outcomes.
Gaume J, Heather N, Tober G, McCambridge J (2018) A Mediation Analysis of Treatment Processes in the UK Alcohol Treatment Trial. Journal of Consulting and Clinical Psychology 86: 321–329
Some MET therapists used MET specific behaviours (motivational interviewing skills) to a high standard, but so did some SBNT therapists.
Quality (not frequency) of motivational interviewing skills predicted 12-month alcohol outcomes, irrespective of treatment condition.
Since both MET and SBNT therapists scored high on MET quality items, this may have contributed to the finding that both interventions have similar outcomes. The table shows the therapist behaviours that predicted drinking outcomes.
The scores for therapists’ use of motivational skils were exctracted from the UKATT Process Rating Scale.
Open questions and complex reflections were associated with ‘preparatory’ talk, that is talk that comes before making a commitment to change.
Complex reflections were predictive of strong client commitment talk, which typically was expressed after a brief delay - perhaps to digest and think over the reflection.
Other motivational techniques did not have effects on commitment to change.
Brown M, Masterson C, Latchford G, and Tober G (2018) Therapist–Client Interactions in Motivational Interviewing: The Effect of Therapists’ Utterances on Client Change Talk. Alcohol and Alcoholism 53: 408-411
When therapist MI consistent behaviour was adopted in response to client resistance talk, it was three times more likely than chance to be followed by change talk, and twice as likely to be followed by ambivalence, a step in between resistance talk and change talk.
MI inconsistent behaviour resulted in more resistance talk, whereas change talk and ambivalence were 50-60% less likely. The findings add support to the causal model.
Drage L, Masterson C, Tober G, Farragher T, and Bewick BM (2019) The Impact of Therapists’ Responses to Resistance to Change: A Sequential Analysis of Therapist Client Interactions in Motivational Interviewing. Alcohol and Alcoholism 54: 173-176
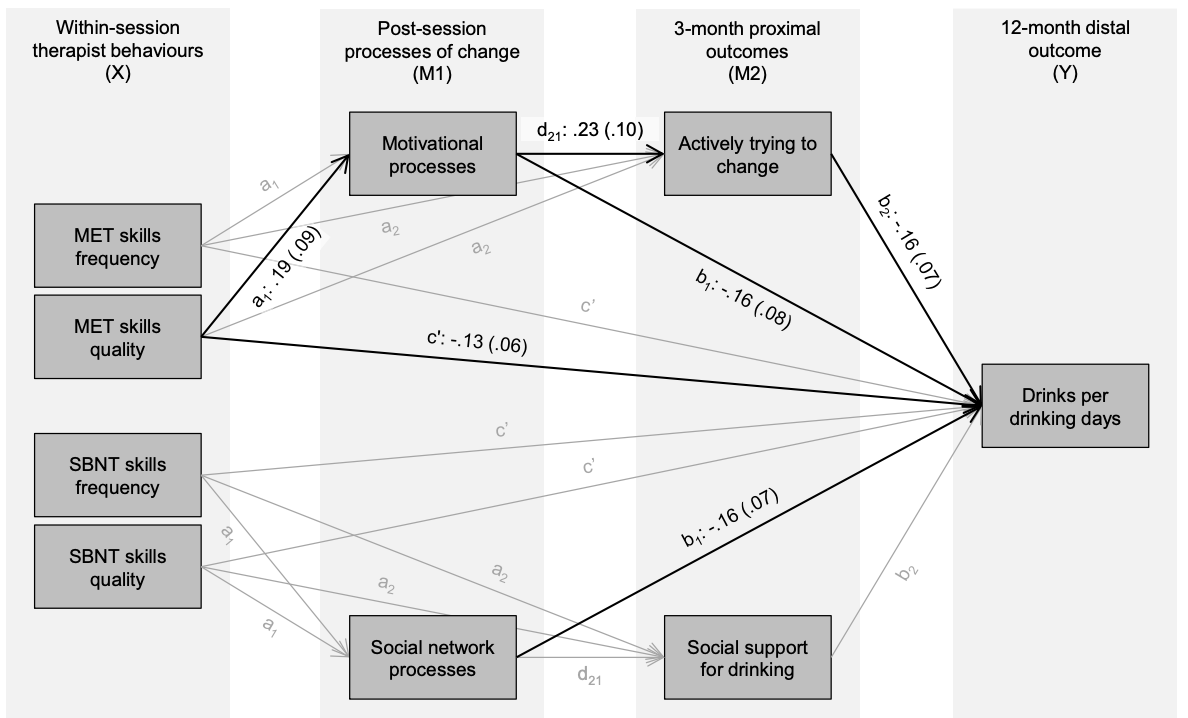
Gaume J, Heather N, Tober G, Studer J, Bedendo A, Raistrick D & McCambridge J (2022) Serial mediation analysis of treatment-specific processes in two contrasting alcohol treatments. Journal of Substance Abuse Treatment 140: 1-7
The serial mediation model (black arrows indicate statistically significant paths and grey indicate non-significant paths)
Quality of MET skills was related to client reported post-session processes of change
Quality of MET skills was related directly to 12-month alcohol outcomes
Higher scores on client reported motivational processes were related to trying to change drinking post-treatment
Trying to change drinking was a strong predictor of lower drinks on a drinking day
Client reported social processes were predictive of treatment outcome in the SBNT group
Significant indirect effects on drinking outcomes were mediated through MET triggering ongoing motivational processes for the client and thereby increasing readiness to change.
The processes of change were measured by a 10-item self-completion rating scale adapted from Project MATCH for UKATT
more for practitioners…